Hospital Humidity Control Calculations in HVAC Design
- nexoradesign.net
- Mar 14
- 7 min read
Introduction

Hospital humidity control calculations are a critical part of healthcare HVAC design because moisture conditions directly affect patient safety, infection control, staff comfort, equipment reliability, and building durability. In hospitals, engineers are not only maintaining temperature; they are also controlling latent heat, pressurization, filtration performance, and condensation risk across spaces with very different functions.
A patient room, sterile processing department, operating room, isolation room, laboratory, and pharmacy all behave differently from a moisture-load perspective. Some spaces need tight humidity limits to reduce microbial growth and protect sensitive procedures, while others generate high internal moisture from occupants, cleaning processes, steam equipment, or outside air ventilation. If the humidity calculation is weak, the system may look acceptable on a simple sensible cooling basis but fail in real operation.
This is why hospital HVAC design must include careful psychrometric analysis, outdoor air latent load evaluation, moisture generation assessment, and coil/dehumidification selection. Good engineering is not just about meeting a dry-bulb setpoint. It is about maintaining stable indoor conditions under worst-case summer, part-load, and shoulder-season conditions. (Hospital Humidity Control Calculations in HVAC Design)
Definition :
Hospital humidity control calculations are the engineering process used to determine the moisture removal or humidification capacity required to maintain indoor relative humidity within design limits in healthcare spaces. These calculations combine outdoor air conditions, ventilation rates, occupancy, internal moisture sources, supply air conditions, and psychrometric relationships to size HVAC equipment and control strategies accurately.
What is Hospital Humidity Control
Hospital humidity control is the management of indoor moisture content so that a healthcare space stays within its required relative humidity range while also maintaining temperature, ventilation, and pressure relationships.
System purpose (Hospital Humidity Control Calculations in HVAC Design)
The purpose of humidity control in hospitals is to:
limit microbial growth and surface condensation
support infection prevention strategies
maintain patient and staff comfort
protect medical equipment and sterile supplies
prevent building material deterioration
Where it is used
Humidity control is especially important in:
operating rooms
isolation rooms
intensive care units
pharmacies
sterile processing departments
laboratories
imaging rooms
inpatient rooms and treatment areas
Why engineers apply it
Engineers apply hospital humidity control calculations to ensure the selected air handling unit, cooling coil, reheat section, humidifier, and control sequence can handle both sensible and latent loads. Without this step, systems can become oversized for sensible cooling but undersized for moisture removal, which often causes high indoor RH during mild-weather operation.
Engineering Principles
Hospital humidity control is based on several core HVAC engineering principles.
Psychrometrics
Humidity calculations depend on psychrometric properties such as:
dry-bulb temperature
wet-bulb temperature
relative humidity
humidity ratio
dew point
enthalpy
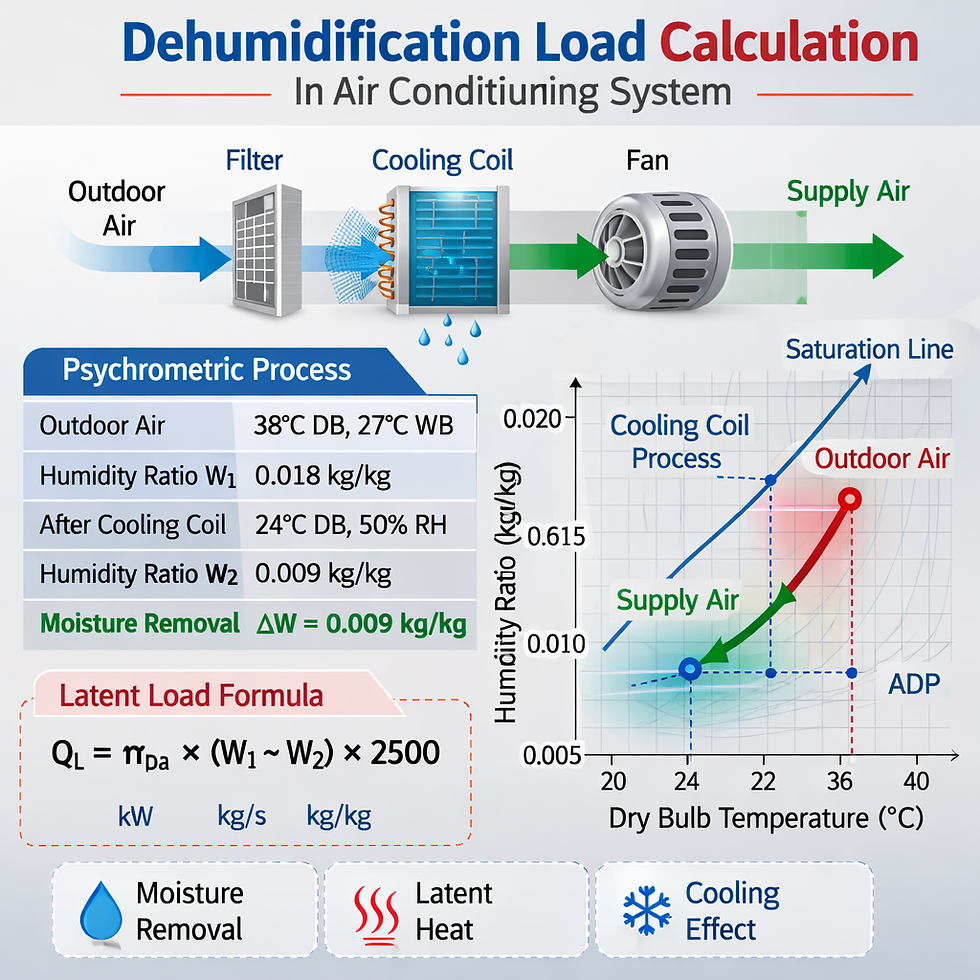
In practice, the engineer converts outdoor and indoor design conditions into humidity ratio values. Moisture transfer is then calculated from the difference in humidity ratio between entering and leaving air states.
Latent heat transfer
Latent load represents the energy associated with adding or removing moisture. In hospital spaces, latent load may come from:
outdoor ventilation air
occupants
steam or hot water processes
open water surfaces
cleaning and sanitation activities
infiltration through envelopes or door openings
Ventilation effect
Hospitals typically require high outdoor air quantities. This makes outdoor air a dominant latent load source, particularly in hot-humid climates. Even when the sensible load is low, the required ventilation may still drive a large dehumidification demand.
Coil apparatus dew point
The cooling coil must cool the mixed air below its dew point so moisture condenses on the coil surface. The coil leaving condition and bypass factor determine how effectively the coil removes latent heat.
Reheat and control stability
Because hospitals may need cool, dry air for moisture removal but neutral supply air for room comfort, reheat is often used after deep cooling. This is common in critical healthcare areas where humidity stability matters more than simple energy minimization.
Step-by-Step Engineering Process
Step 1 – Establish design criteria
Define the required room conditions:
indoor design dry-bulb temperature
target relative humidity range
room pressure relationship
minimum air changes per hour
minimum outdoor air requirement
For example, a critical room may need 22°C and 50% RH with a permitted range based on project criteria, local code, and healthcare guidelines.
Step 2 – Determine moisture loads
Calculate all latent contributors:
outdoor air ventilation load
occupant latent gain
infiltration
process moisture
building-related moisture migration
A common ventilation latent load method is:
Latent moisture load = Airflow × air density factor × (W_outdoor - W_indoor)
Where:
airflow is the outdoor air quantity
W is humidity ratio in kg/kg dry air or grains/lb depending on unit system
For quick SI moisture mass flow estimation:
Moisture removal rate = 1.2 × Airflow (m3/s) × (W1 - W2)
This gives approximate kg/s of moisture condensed when the units are consistent.
Step 3 – Select supply air state
Choose the required supply air humidity ratio low enough to offset room latent load. This is not based only on supply temperature. The supply dew point must be low enough to maintain room RH under design occupancy and ventilation conditions.
Typical questions include:
Does the coil leaving air need to be 10°C, 12°C, or lower?
Is reheat required?
Is a dedicated outdoor air system needed?
Step 4 – Verify coil and control sequence
After selecting the AHU coil, verify performance at:
peak summer design
part-load sensible conditions
high ventilation / low sensible conditions
morning warm-up or high-occupancy transitions
This is where many hospital systems fail. The coil may meet peak load but lose humidity control at part load if airflow reduction or chilled water reset is not evaluated.
Practical Engineering Example
Consider a hospital operating suite served by an AHU with these simplified design conditions:
Outdoor air: 35°C DB, 24°C WB
Room design: 22°C, 50% RH
Total supply airflow: 5.0 m3/s
Outdoor air portion: 1.5 m3/s
Occupants: 12 persons
Occupant latent gain: 55 W/person
From the psychrometric chart, assume:
Outdoor humidity ratio = 0.017 kg/kg
Room humidity ratio = 0.0082 kg/kg
1. Outdoor air moisture load
Moisture mass flow from outdoor air to room condition basis:
1.2 × 1.5 × (0.017 - 0.0082)
= 1.8 × 0.0088= 0.01584 kg/s moisture
That equals:
0.01584 × 3600 = 57.0 kg/h of moisture
2. Occupant latent load
12 × 55 = 660 W latent
Using latent heat of vaporization around 2500 kJ/kg:
0.66 kW / 2500 kJ/kg
= 0.000264 kg/s
= 0.95 kg/h moisture
The outdoor air dominates the latent load, which is typical in healthcare systems.
3. Total estimated latent moisture removal
Total moisture removal required is approximately:
57.0 + 0.95 = 57.95 kg/h
This excludes infiltration or process moisture, so real design value may be higher.
4. Coil leaving condition implication
To maintain the room at 50% RH, the supply air humidity ratio must be below room humidity ratio. Suppose the coil leaves at W = 0.0070 kg/kg. The supply air can then absorb room latent load while offsetting ventilation-driven moisture rise.
This example shows the design lesson clearly: hospital humidity control is usually ventilation-driven first, occupancy-driven second, and temperature-only thinking is not enough.
Technical Comparison Table
Approach | Humidity Control Accuracy | First Cost | Energy Use | Best Use Case | Main Limitation |
Standard chilled water AHU only | Moderate | Low | Moderate | General hospital areas | Weak at part-load dehumidification |
AHU with deep cooling and reheat | High | Medium | High | Critical areas with stable RH needs | Reheat energy penalty |
DOAS + local terminal units | High | Medium-High | Efficient when optimized | Large hospitals with ventilation separation | More complex control integration |
Desiccant-assisted dehumidification | Very High | High | Medium-High | Hot-humid climates, high latent load zones | Higher capital and maintenance complexity |
Heat pipe / wrap-around coil assist | Moderate-High | Medium | Lower than electric reheat | Retrofit moisture control improvements | Limited flexibility compared with full DOAS |
Advantages
Accurate hospital humidity control calculations provide several engineering benefits:
improved compliance with healthcare environmental requirements
lower risk of condensation on diffusers, ducts, and ceilings
better infection-control support
improved comfort for patients and staff
protection of sterile materials and medical devices
more reliable AHU and coil sizing
fewer post-occupancy control problems
reduced mold and moisture-related building damage
Common Engineering Mistakes
The most common mistakes include:
sizing the system using sensible load only
ignoring the latent impact of minimum outdoor air
assuming VAV turndown will still maintain dehumidification
selecting supply temperature without checking supply humidity ratio
not reviewing shoulder-season or part-load humidity behavior
omitting reheat where deep dehumidification is required
using generic office-building assumptions for healthcare areas
failing to coordinate humidity control with pressure relationships and filtration
A frequent real-world issue is chilled water reset combined with reduced coil performance. Energy strategies that look efficient on paper can cause indoor RH drift unless moisture control logic is protected.
Future Trends
Hospital HVAC humidity control is evolving toward more intelligent and resilient systems.
AI-assisted control optimization
Advanced analytics can detect humidity drift patterns, coil inefficiency, valve hunting, or sensor bias before they become patient-area issues.
Digital twin integration
Digital twins allow engineers and facility teams to compare live hospital conditions with design intent, especially in critical airside systems.
Better decoupled ventilation strategies
DOAS-based healthcare designs are gaining attention because they separate outdoor air moisture control from zone sensible control.
Sensor quality and continuous commissioning
More projects are using continuous monitoring of dew point, RH, pressure, and valve position to maintain healthcare HVAC performance over time.
Energy-aware dehumidification
Future designs will balance humidity stability with lower energy use through heat recovery, adaptive reset strategies, and high-performance coil configurations.
FAQ Section
1. Why is humidity control more difficult in hospitals than in offices?
Hospitals require higher outdoor air quantities, tighter pressure control, and more critical room conditions. These factors make latent load management much more demanding than in standard commercial buildings.
2. What is the main source of latent load in hospital HVAC systems?
In many hospital applications, the main source is outdoor ventilation air, especially in hot-humid climates. Occupants and processes add load, but outside air often dominates.
3. Can a low room temperature alone control humidity?
No. Humidity depends on moisture content, not just dry-bulb temperature. A room can feel cool while still having excessive RH if the supply air dew point is not low enough.
4. When is reheat necessary in hospital humidity control?
Reheat is often necessary when the system must cool air deeply to remove moisture but cannot deliver overly cold air directly to occupied spaces.
5. Should hospital humidity control be checked at part load?
Yes. Many failures happen at part load, not peak summer load. Reduced sensible cooling demand can reduce coil dehumidification unless the control sequence is designed properly.
Conclusion
Hospital humidity control calculations are one of the most important parts of healthcare HVAC engineering because they connect psychrometrics, infection-control support, ventilation, and equipment performance into one design problem. Engineers must calculate latent loads carefully, especially from outdoor air, then select a supply air condition and coil performance that can maintain indoor RH under both peak and part-load conditions.
The best hospital designs do not treat humidity as a secondary issue after temperature control. They treat moisture management as a primary design parameter from the first load calculation through final control sequence review. When that happens, the result is a safer, more stable, and more reliable healthcare environment.
Author Note :
Nexora Design Lab publishes engineering insights on HVAC design, MEP systems, and sustainable building technologies used in modern construction projects.


Comments